

Abstract

Background. Arterial occlusive events (AOEs) represent emerging complications in chronic myeloid leukemia (CML) patients treated with ponatinib, with a cumulative incidence correlated with the higher dose of the drug and longer treatment duration. Current recommendations highlight the importance of a careful evaluation of cardiovascular (CV) risk factors at baseline.Moreover, a preventive strategy with primary prophylaxis based on aspirin still remains under discussion and no data have been reported on secondary prophylaxis.
Methods.We investigated a consecutive series of adult CML patients (mean age 50 years, range 24-81) who initiated ponatinib, between January 2012 and December 2016 at 15 Italian centers. Patients were stratified according to the Systematic Coronary Risk Evaluation (SCORE) assessment, based on gender, age, smoking habits, systolic blood pressure, and total cholesterol levels. Additional risk factors were considered the presence of diabetes, body mass index > 24.5 kg/m2, mild or severe renal insufficiency, and dyslipidemia. CML patients were also evaluated for both comorbidities and a positive anamnesis of CV diseases.Primary and secondary CV prophylaxis before starting ponatinib was also reported. We evaluated the cumulative incidence of AOEs (myocardial infarction, angina, ischemic cerebrovascular events and peripheral vascular disease) after initiating treatment with ponatinib, and their management.
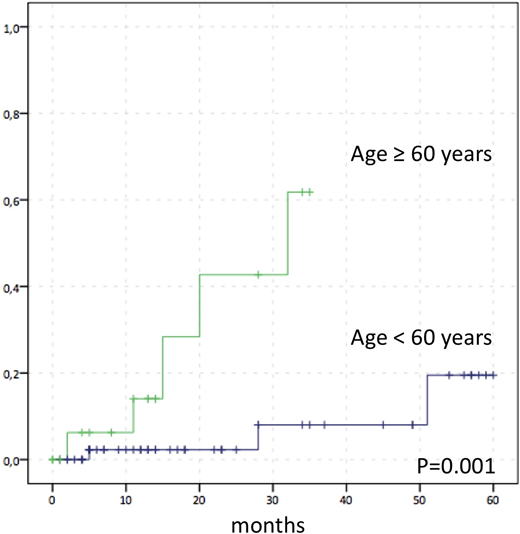
Results.A total of 71 patients were retrospectively identified. The reasons for treatment with ponatinib were inefficacy of previous tyrosine kinase inhibitors (TKIs) in 80.2% and intolerance in 19.8%. The median time of exposure to ponatinib was 16 months (range 3-69).The 60-month cumulative incidence of AOEs was 30.9±11.5%.Patients aged ≥60 years showed a higher incidence of AOEs (61.8±19.5% vs 19.5±12.0%, p=0.001) (Figure 1). The majority of patients (95%) were classified as at low-intermediate SCORE risk and 5% as at high-very high SCORE risk. Patients with a high-very high SCORE showed a significantly higher incidence of AOEs (100% vs. 25.8±11.5%; p<0.002). In multivariate analysis, no association was found with positive anamnesis of CV diseases, CV risk factors, dose of ponatinib (15, 30, 45 mg), exposure time to ponatinib, and number of TKI treatments; only age ≥60 years showed a significative association (p=0.016) . Overall, 13 patients underwent aspirin 100 mg primary prophylaxis before starting ponatinib and showed a a lower albeit not statistically significant incidence of AOEs (14.3±13.2% vs 33.4±12.8%, p=NS). In 6 of these patients with age < 60 years, no AOEs was reported. Conversely, the cumulative incidence of AOEs in the 6 patients undergoing secondary prophylaxis (anticoagulant, cardioaspirin) for previous events was 100% at 30 months. Overall, 23 CV AEs were registered; 52.1% of CV AEs were graded as 3/4 according to common toxicity criteria. In 43.4% of cases, ponatinib treatment did not require dose modification, 34.8% of patients reduced the dose and 21.8% discontinued the treatment. The majority of patients required additional diagnostic tests as ECG/cardiac ultrasound, peripheral vascular Doppler or cranial/CT; 4 patients underwent a coronarography procedure and 1 patient required invasive procedures as percutaneous transluminal angioplasty and application of coronary stents. Finally, the 5-year cumulative incidence of MR4 following ponatinib treatment was 45.0±12.3% and it was not influenced significantly by AOEs occurrence.
Conclusions.This study confirms the increased risk of AOEs in CML patients treated with ponatinib in the real-life, particularly in patients aged ≥60 years. Our findings emphasize the need of personalized prevention strategies based on CV risk factors, in close collaboration with cardio-oncologists, angiologists and vascular surgeons. We suggest that patients treated with ponatinib should undergo prophylaxis with aspirin 100 mg. Data on the efficacy of primary prophylaxis need to be confirmed in larger cohorts of patients and in prospective randomised trials.
Figure 1.Arterial Occlusive Events (AOEs) cumulative incidence according to age ≥ 60 years in 71 CML patients treated with ponatinib
Abruzzese:BMS: Consultancy; Novartis: Consultancy; Ariad: Consultancy; Pfizer: Consultancy. Bonifacio:Incyte: Consultancy; Pfizer: Consultancy; Amgen: Consultancy; Novartis: Research Funding; Bristol Myers Squibb: Consultancy. Foà:CELTRION: Other: ADVISORY BOARD; GILEAD: Speakers Bureau; ABBVIE: Other: ADVISORY BOARD, Speakers Bureau; CELGENE: Other: ADVISORY BOARD, Speakers Bureau; NOVARTIS: Speakers Bureau; ROCHE: Other: ADVISORY BOARD, Speakers Bureau; INCYTE: Other: ADVISORY BOARD; AMGEN: Other: ADVISORY BOARD; JANSSEN: Other: ADVISORY BOARD, Speakers Bureau. Breccia:Incyte: Honoraria; BMS: Honoraria; Novartis: Honoraria; Pfizer: Honoraria.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal